
Manipulation Under Anaesthetic (MUA) When to decide to take the next step?
Knee Stiffness After Total Knee Replacement
When Is a Manipulation Under Anaesthetic Needed?
Knee replacement surgery is designed to improve pain and function — but for some patients, stiffness becomes the biggest barrier to recovery.
Instead of feeling better, the knee feels:
Tight
Restricted
Difficult to bend or straighten
And in some cases, progress seems to stop altogether.
How Common Is Knee Stiffness?
Knee stiffness after a total knee replacement is a recognised complication.
Research suggests:
Around 1–6% of patients develop significant stiffness that impacts function
A subset of these patients require further intervention
Approximately 2–6% of all knee replacement patients undergo a manipulation under anaesthetic (MUA)
👉 In real-world terms:
Most patients recover well — but a small group develop stiffness that needs extra help.
What Causes Knee Stiffness?
The most common cause is arthrofibrosis — excessive scar tissue forming inside and around the joint.
This can lead to:
Reduced range of motion
Pain with movement
A feeling of the knee being “blocked”
Stiffness is rarely due to just one factor. It is usually multifactorial, including:
Pre-existing stiffness before surgery
High levels of inflammation and swelling
Pain limiting early movement
Delayed or limited rehabilitation
Individual healing responses (some people scar more aggressively)
When Is a Manipulation Under Anaesthetic (MUA) Needed?
A Therapist’s Perspective: Not All Stiff Knees Are the Same
From a therapist’s point of view, one of the most important distinctions we make is how the knee feels when we try to move it.
Some patients are limited primarily by pain.
The knee feels tight, guarded, and uncomfortable — but there is still a sense that it could move further.
👉 These patients often improve over time with the right rehab, good pain control, and gradual progression.
But other knees feel very different.
👉 There is a firm, hard block — a point where the joint simply will not move any further, no matter how much effort is applied.
This type of stiffness is more suggestive of a mechanical restriction, often related to scar tissue (arthrofibrosis), rather than just pain.
Why This Matters for the MUA Decision
This distinction is critical when deciding whether to proceed with an MUA.
Pain-limited knees → often improve with time and continued rehab
Mechanically blocked knees → are less likely to change without intervention
👉 This is where clinical experience becomes incredibly important.
An experienced physiotherapist can recognise when:
Progress is still being made (even if slow)
Or when the knee has genuinely plateaued and is unlikely to improve further without assistance
A manipulation under anaesthetic is considered when:
👉 Range of motion is not improving despite appropriate rehab
Common clinical triggers include:
Difficulty bending beyond ~90 degrees
Inability to fully straighten the knee
Progress plateauing in the first 6–12 weeks
Most surgeons will consider MUA:
👉 Within the first 6–12 weeks after surgery
(as outcomes tend to be better when done earlier)
However, research shows it can still be effective later in some cases .
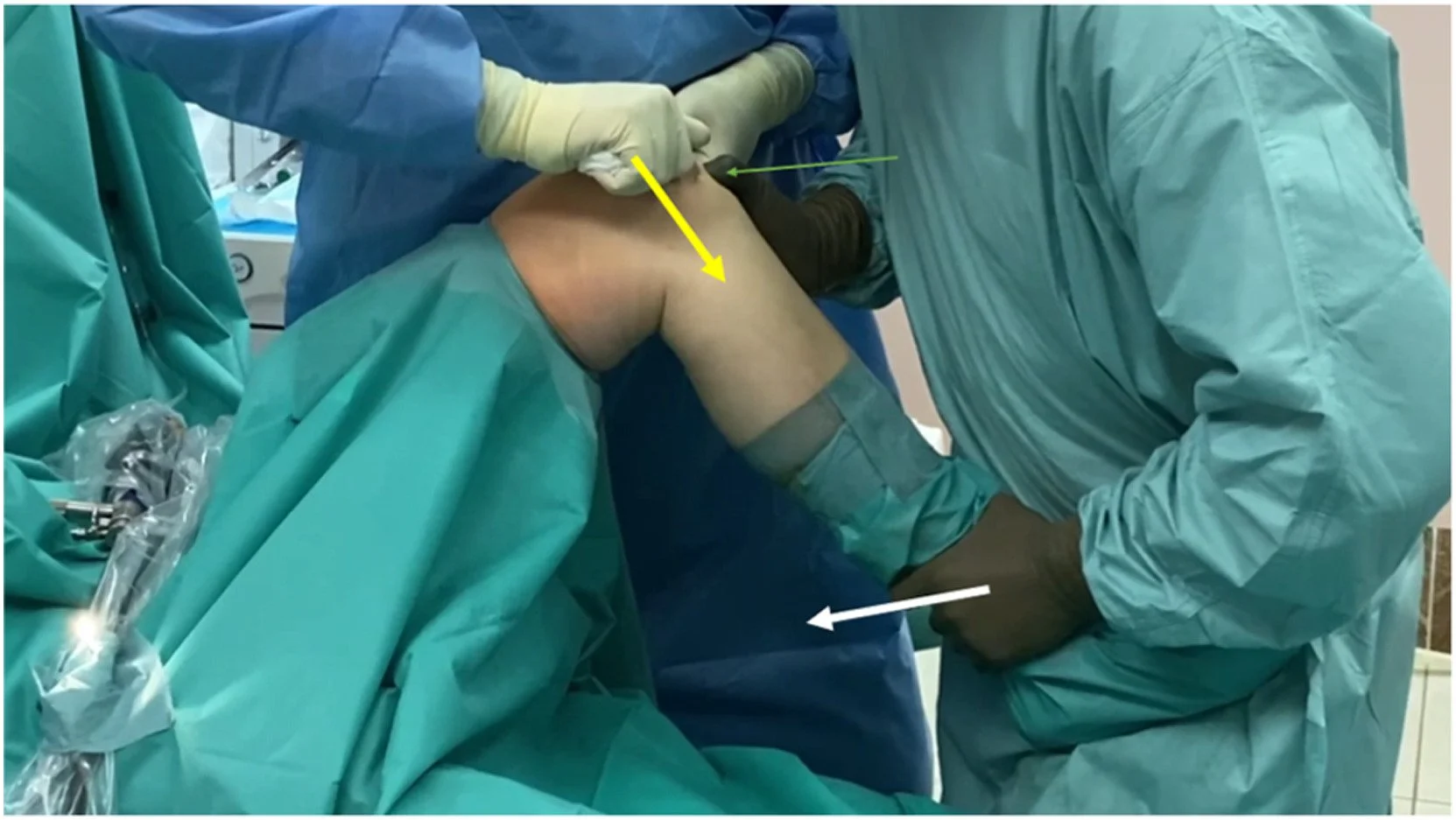
What Does the Procedure Involve?
An MUA is a relatively quick and minimally invasive procedure.
You are placed under anaesthetic (so you feel no pain)
The surgeon gently but firmly moves the knee through its range
This helps break up scar tissue adhesions restricting movement
👉 There are no incisions made — the goal is to restore motion without further surgery.
Does It Work?
In many cases, yes.
Research shows:
Patients often gain 10–30+ degrees of movement following MUA
It can help avoid more invasive surgery
It is generally considered safe and effective as a first-line treatment for stiffness
However:
👉 It is not a magic fix — outcomes depend heavily on what happens next.
What Happens After MUA? (This Is Critical)
The procedure itself is only part of the solution.
👉 Rehabilitation immediately afterwards is essential
Without proper follow-up, stiffness can return.
Post-MUA rehab typically includes:
Early and frequent physiotherapy
Aggressive (but controlled) range of motion work
Strengthening exercises
Swelling management
Regular movement throughout the day
👉 The window after MUA is crucial — this is when the knee is most responsive to change.
Why Some Patients Still Struggle
Even after MUA, some patients continue to experience stiffness.
This may be due to:
Ongoing inflammation
Persistent pain limiting movement
Reformation of scar tissue
Underlying movement or strength deficits
In some cases, further procedures (like arthroscopic scar tissue removal or revision surgery) may be considered — but this is less common.
In clinic, knee stiffness can be one of the most frustrating complications we see.
Patients often say:
“I feel like I’m doing everything right, but it’s not improving”
“My knee just won’t bend”
And importantly:
👉 This is not always the patient’s fault.
Some people simply have a stronger scar tissue response or a more difficult recovery pathway.
Key Takeaways
✔️ Knee stiffness is an uncommon but important complication
✔️ Around 2–6% of patients may need a manipulation under anaesthetic
✔️ Early identification and treatment lead to better outcomes
✔️ MUA can significantly improve movement
✔️ Rehab after MUA is just as important as the procedure itself
Final Thought
A stiff knee after replacement can feel like a setback — but it’s not the end of the road.
With the right timing, the right intervention, and the right rehab plan:
👉 Significant improvements are still possible
Struggling with knee stiffness after your knee replacement?
If your progress has plateaued or your knee isn’t bending the way it should:
👉 Book an assessment — we’ll help you understand what’s going on and map out the next steps for your recovery.